He has studied microsurgical techniques and the art of plastic surgery. Dr. Afra studied medicine at UCLA, where he also completed his surgery internship. Prior to attending medical school, Dr. Afra worked at the Salk Institute on an NIH research stipend. In 2010, Dr. Robert Afra was selected by the Arthroscopy Association of North America, a premiere sports medicine society, as one of three surgeons to lecture to university faculty in the United States and Canada.
Rob lives in Solana Beach with his wife Johanna and their three children, Aviya, Mycah and Jean-Raphael. In his free time, he enjoys traveling, jiujitsu, skiing, campouts with the Adventure Guides and Princess tribes, biking along the beach with family, early morning runs along the Coast, and trying to stay awake long enough to finish reading to his kids at bedtime!
CLASSIC LIST

Dr. Robert Afra is a widely respected leader in San Diego orthopedic surgery. The former Chief of Sports Medicine at the University of California, San Diego, Dr. Afra has published extensively in professional journals and books and presented at conferences around the world, where he is considered a pioneer in the study of shoulder, knee, elbow and ankle injuries in athletes and active adults. Dr. Afra is also a specialist in cartilage issues and pain in knee cap disorders, and was named Co-Director of the International Patellofemoral Study Group Conference in San Diego in July 2011. Dr. Afra completed his fellowship training in sports medicine at Boston University, where he treated a variety of elite college athletes in ice hockey, soccer, basketball, field hockey and lacrosse.
Dr. Afra was a researcher at University of Hawaii’s Queen Emme Medical Center in the field of muscle and nerve physiology, and was a surgical fellow at the world-renowned Barnard O’Brien Microsurgical Institute in Melbourne, Australia.
Shoulder pain and impaired movement can be debilitating symptoms. Click here to learn more about our safe

Osteoarthritis Often Gets Worse Before Knee Replacement
A study has found that many osteoarthritis patients who receive knee replacements had increasingly severe symptoms in the months leading up to their surgeries.
Knee replacement (also known as total knee arthroplasty or TKA) entails replacing the joint with metal or plastic prosthetic devices. Orthopedic surgeons sometimes recommend the operation as the best option, when the pain and stiffness of knee arthritis makes walking and other everyday activities difficult.
The multicenter study, reported by Daniel Riddle and William Jiranek of Virginia Commonwealth University in “Osteoarthritis and Cartilage,” was the subject of a recent Medpage Today article.
The research indicated that nearly a third of those who had TKA “experienced rapid disease progression and worsening of osteoarthritis symptoms” during the two years before their operations.
The patients’ Kellgren and Lawrence grade became worse in 27.4 percent of the cases. That was true for only 6.6 percent of knee osteoarthritis sufferers who did not have TKA. The grade’s four-part scale measures the extent of symptoms. Grade 1 is “doubtful narrowing of joint space.” Grade 4, identified in the most extreme cases, involves “large osteophytes (bony outgrowths), marked narrowing of joint space, severe sclerosis (abnormal hardening of body tissue) and definite deformity of bone contour.”
 The researchers noted that 45.6 percent of knees with grades lower than four exhibited “radiographic progression.” The patients’ WOMAC function and Knee Injury and Osteoarthritis Outcome Scores (KOOS) confirmed that symptoms can intensify before TKA. Patients who did not undergo knee replacements saw their scores stay the same or improve during the two-year period. The two measurement methods assess the degree of knee pain, stiffness and function.
The researchers noted that 45.6 percent of knees with grades lower than four exhibited “radiographic progression.” The patients’ WOMAC function and Knee Injury and Osteoarthritis Outcome Scores (KOOS) confirmed that symptoms can intensify before TKA. Patients who did not undergo knee replacements saw their scores stay the same or improve during the two-year period. The two measurement methods assess the degree of knee pain, stiffness and function.
Medpage Today pointed out that “these findings run counter to the traditional suggestion that knee osteoarthritis is a slowly progressive disorder.”
The authors of the study wrote: “This high rate of radiographic worsening, and associated pain and functional status worsening, in our view, likely contributes to surgeons’ recommendations and patients’ decision to opt for TKA.” They called for additional research, explaining that “the path toward TKA for persons with osteoarthritis is an understudied and relatively poorly understood process.”
The researchers used data from the Osteoarthritis Initiative (OAI) and the National Institute of Health to arrive at their conclusions. They examined the records of nearly 5,000 patients who were enrolled in OAI. Of those, 167 underwent TKA. X-rays and other diagnostic tests were performed for five years, before and after the patients’ surgeries.

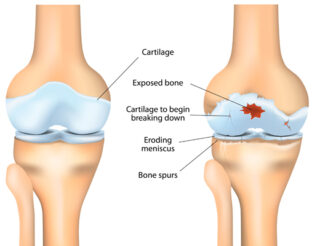
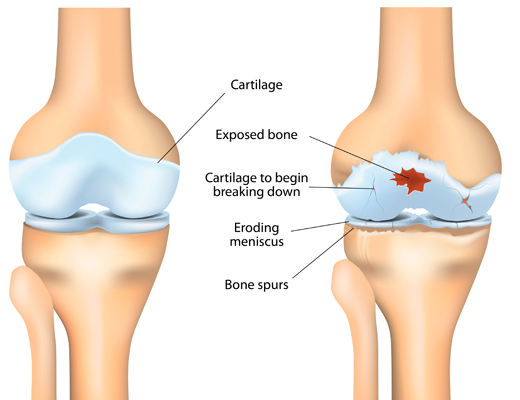
Osteoarthritis is the most common form of knee arthritis, according to the American Academy of Orthopaedic Surgeons. The organization describes the condition as “a degenerative, wear-and-tear type of arthritis that occurs most often in people 50 years of age and older, but may occur in younger people.”
Cartilage that cushions bones in the joint gradually deteriorates, becoming rough and frayed. That decreases the space between the bones, resulting in them rubbing against one another. Bone spurs sometimes develop, causing additional pain.
If you have knee pain and stiffness, the best thing to do is get a diagnosis to determine whether you have osteoarthritis. Treatments ranging from medications to knee replacement (total knee arthroplasty) are available. Schedule an evaluation by the sports medicine staff at Orthopedic Surgery San Diego to learn about your options.
ENERGY DRINKS – A DANGEROUS MIX FOR YOUNG CHILDREN.
 Exposure to energy drinks is an on-going health problem.
Exposure to energy drinks is an on-going health problem.
The potential dangers of energy drinks, the caffeine-rich beverages which promise a super-human boost, are very well-known. However, recent studies have shown that even young children are now at risk.
Although the target market for energy drinks is usually teenagers and adults, the US poison control reported that over a measured time period, about 40% of emergency calls received concerned children under the age of 7. A few of the more serious cases involved seizures and abnormal heart rhythms. Of course, most of these children had no idea what they were drinking.
How do these young kids get hold of the energy drinks they consume?
Many people, including parents, are unaware of the potential for energy drinks to have serious side effects. A child cannot go into a store and purchase an energy drink. They are usually easily accessible in the home refrigerator where the drinks are kept by parents or older siblings who do not recognise the dangers posed.
Any child will be attracted by the attractive packaging and coloring of the drinks and if accessible, happily consume it. Many parents will be blissfully ignorant that this has taken place, until some unpleasant side effects occur.y
Underlying health issues.
Children with less obvious conditions such as borderline diabetes or attention deficit hyperactivity disorder, will suffer a much greater negative impact from caffeinated energy drinks than that of healthy children.
Some energy drinks have up to 400mg caffeine per serving, compared to the average cup of coffee which contains about 100 to 150mg. It has been noted that caffeine poisoning can occur at a level of 400mg and up, for adults.
For a child this could have a potential deadly effect.
Is something being done to promote awareness of dangers posed to young children?
The American Beverage Association has stated that caffeinated energy drinks are not intended for consumption by the very young. In fact, leading energy drink makers voluntarily place statements on their packaging and labelling to the effect that the products are not intended for children. Although this does help, it is generally felt by concerned health professionals that more needs to be done to create awareness.

What can YOU do to help your kids?
Research has shown that children who lead an active lifestyle, exercise regularly and have a healthy, nutritious diet have absolutely no need of energy drinks. Parents, teachers and coaches need to focus on the use of water to replenish fluids after sports or exercise. Nutritious drinks such as fruit juice or low-fat milk should be encouraged at mealtimes or at group outings.
If you are a parent who consumes energy drinks, make certain that they are not stored any place where the drinks will be accessible to your kids. If they are too young to go into a store to buy the drinks, the only access will be through you if you are careless.
Continue to promote a healthy and nutritious lifestyle for your family, and lobby to reduce the marketing and availability of energy drinks to children.
Positive Meniscal Lesions: A Strong Predictor of Neuropathic Pain in Osteoarthritis
Osteoarthritis (OA) is the most common form of arthritis, with the knees, spine, hips, and hands as the usual site of affectation. OA occurs when the ligament, a structure that protects the ends of bones, wears down. This may be attributed to aging and prolonged use. There is no cure and the pain is severe it can greatly affect people’s activities of daily living. In addition to this, OA predisposes people to disabilities such as fractures, contractures, and knee injury, among others.
Basically, pain is acknowledged to be caused by damage in the structure of the joints affected. However, there is a disparity between the symptoms reported by patients and the structural picture taken by imaging studies, which is currently the mainstay diagnostic test. With the belief that other factors contribute to pain, a study entitled, “The presence of meniscal lesions is a strong predictor of neuropathic pain in symptomatic knee osteoarthritis: a cross-sectional pilot study” was conducted by a group of researchers in Canada led by Camille Roubille. The aim of the study was to explore the relationship between structural changes and presence of neuropathic pain (NP) in patients with symptomatic knee OA. The study was published online on December 2014 in BioMed Central (BMC).
 Subjects involved were 40 years old and older with symptoms of OA for at least one month out of three months before the study was conducted. These patients are diagnosed with primary knee OA and with radiological grades 2 and 3 according to Kellgren-Lawrence (KL) criteria. Aside from this, subjects included had a visual analog scale (VAS) of 40 mm or greater while walking on a flat surface. Subjects who did not meet the criteria before, during, and after the study were excluded. In addition, those with other diagnosed medical conditions affecting knee function, isolated knee OA, have participated in other investigational study within 30 days prior to becoming subject, and have taken steroids were not included. Presence of NP was determined using PainDETECT questionnaire and 50 knee OA patients were divided into two groups: 1) 25, for those with unlikely NP; and 2) those with uncertain or likely NP. None of these patients received treatments for NP such as antidepressants and anticonvulsants.
Subjects involved were 40 years old and older with symptoms of OA for at least one month out of three months before the study was conducted. These patients are diagnosed with primary knee OA and with radiological grades 2 and 3 according to Kellgren-Lawrence (KL) criteria. Aside from this, subjects included had a visual analog scale (VAS) of 40 mm or greater while walking on a flat surface. Subjects who did not meet the criteria before, during, and after the study were excluded. In addition, those with other diagnosed medical conditions affecting knee function, isolated knee OA, have participated in other investigational study within 30 days prior to becoming subject, and have taken steroids were not included. Presence of NP was determined using PainDETECT questionnaire and 50 knee OA patients were divided into two groups: 1) 25, for those with unlikely NP; and 2) those with uncertain or likely NP. None of these patients received treatments for NP such as antidepressants and anticonvulsants.
Demographic data, VAS and Western Ontario and McMasters Universities Osteoarthritis Index (WOMAC) scores, PainDETECT questionnaire results, blood tests for inflammatory markers (e.g. sedimentation rate and C-reactive protein), and knee x-rays were done.
It was found out that higher WOMAC score which reflects increasing pain, function, and stiffness is associated with higher VAS and PainDETECT score. However, biomarkers are not associated with higher PainDETECT score. With regards to structural changes, cartilage volume and synovial membrane thickness are not associated with pain. However, meniscus tear or lesions in meniscus (a C-shaped cartilage that holds both upper and lower leg), both the medial and lateral portion, was found to be significantly associated with increasing PainDETECT scores. This is also true with bone marrow lesions in the lateral portion. In summary, meniscal lesions are a ‘definite major risk factor for NP’.
Researchers recommend conducting a randomized controlled trial (RCT) version of this observational study. Also, experts in sports medicine may develop a gold standard for diagnosing NP since PainDETECT is the only available option.
If you have been told that you have a meniscal tear or are in need of an arthroscopy, schedule an appointment to undergo an evaluation with our sports medicine orthopedists.

Injections More Effective Than Pills in Reducing Knee Osteoarthritis Pain Injections of hyaluronic acid relieve the pain of knee osteoarthritis better than nonsteroidal anti-inflammatory pills, according to an analysis published by the Annals of Internal Medicine. Researchers looked at studies that measured the comparative effectiveness of acetaminophen, diclofenac, ibuprofen, naproxen and celecoxib (Celebrex) pills versus injections of corticosteroids or hyaluronic acid. Some of the clinical trials’ volunteers were given oral or injected placebos. Scientists assessed how the various treatments relieved knee pain, restored function and reduced stiffness. The findings provide important information for the millions of knee osteoarthritis patients who require orthopedists’ services every year. An increasingly popular treatment method features injections of cortisone or hyaluronic acid. In advanced cases, some patients need total knee replacement (also known as knee arthroplasty), which entails surgically replacing the joint with prosthetic devices. The scientists reviewed 137 studies involving 33,243 participants. They concluded that hyaluronic acid was “the most efficacious treatment” for pain, while acetaminophen was the least effective. There was no clear winner in terms of enhancing knee function or reducing stiffness. The researchers wrote: “Intra-articular treatments were superior to nonsteroidal anti-inflammatory drugs. … All treatments except acetaminophen showed clinically significant improvement from baseline pain.”
The authors of the review, funded by the the Agency for Healthcare Research and Quality, were Drs. Raveendhara R. Bannuru, Christopher H. Schmid, David M. Kent, Elizaveta E. Vaysbrot, John B. Wong and Timothy E. McAlindon. Bannuru, a researcher at Tufts Medical Center in Boston, told the New York Times that the best kind of treatment depends upon the individual. He explained: “The key message is that hyaluronic acid and steroid injections are more effective than drugs. But all the harms and benefits need to be taken into account. I would advise people to talk to their physicians about the pros and cons, and choose the treatment appropriate for them.” The knee contains hyaluronan, a gel-like substance that lubricates the joint and acts like a shock absorber during exercise. Osteoarthritis patients have low levels of this material, resulting in irritation. Hyaluronic acid, which has a similar structure as the naturally occurring substance, can be injected into the knee in a procedure called viscosupplementation. Knee osteoarthritis is one of the most common types of arthritis, according to the American Academy of Orthpaedic Surgeons (AAOS). It results from the gradual wearing away of cartilage, which becomes rough and frayed. That increases the space between bones in the joint, causing the bones to rub against each other and sometimes fostering the growth of bone spurs. The condition starts slowly, with the discomfort intensifying over the years. Pain, inflammation and reduced range of motion are the primary symptoms. Knee osteoarthritis limits a person’s ability to perform simple tasks like walking and climbing stairs, and is a leading cause of disability. The condition affects primarily older people, especially those who are sedentary and overweight.

“Vigorous activity may cause pain to flare up,” the AAOS explains on its website. “Loose fragments of cartilage and other tissue can interfere with the smooth motion of joints. The knee may ‘lock’ or ‘stick’ during movement. It may creak, click, snap or make a grinding noise (crepitus). Pain may cause a feeling of weakness or buckling in the knee. Many people with arthritis note increased joint pain with rainy weather.” There is no cure for osteoarthritis. Orthopedists recommend that patients eat a nutritious diet and lose weight. It is also crucial to stop or reduce physical activities that aggravate symptoms. The AAOS advises that “switching from high-impact activities (like jogging or tennis) to lower-impact activities (like swimming or cycling) will put less stress on your knee.” Physical therapy involves individually designed exercises that improve flexibility and expand the knee’s range of motion, while strengthening muscles that support the joint. Among the assistive devices for osteoarthritis sufferers are canes, shock-absorbing shoes and inserts, knee braces and sleeves, and elastic bandages.

Other remedies, according to the AAOS, are applications of heat or ice, pain-relieving ointments or creams, acupuncture, magnetic pulse therapy, glucosamine and chondroitin sulfate supplements, and pain-relief and anti-inflammatory medications. Corticosteroids, also called cortisone, are anti-inflammatory drugs that doctors inject directly into arthritic joints to provide temporary relief. When nonsurgical treatments fail to relieve the pain and restore knee function, cartilage grafting is an option. It involves extracting healthy tissue from another part of the knee and inserting it into the space that contained damaged cartilage. In a procedure known as an osteotomy, the shinbone or thighbone is cut and reshaped to reduce pressure on the knee. When knee replacement (or arthroplasty) becomes necessary, doctors make small incisions in the skin. They insert tiny medical instruments that diagnose the problem, remove damaged cartilage and bone, and implant metal or plastic prosthetics. If you are suffering from pain and reduced function in your knee, it is vital to find out whether your symptoms are caused by osteoarthritis or another condition. Schedule an evaluation by the sports medicine staff at Orthopedic Surgery San Diego to get a diagnosis and learn about the best treatment options available to you.
